
Biomedical
Communication
Biosci. Biotech. Res. Comm. 9(3): 335-340 (2016)
HMGA1 variant IVS5-13insC is associated with
insulin resistance and type 2 diabetes: An updated
meta-analysis
Qinglu Wang
1
* Yancheng Liu
1
Liting Zheng
1
Hao Kong
1
and Xuewen Tian
2
1
Key Laboratory of Biomedical Engineering & Technology of Shandong High School, Qilu Medical
University, Zibo, 255213, China
2
S ports Science Research Center of Shandong Province, Jinan, 250102, China
ABSTRACT
High-mobility group A1 (HMGA1) polymorphism has been suspected as a gene variant associated with type 2 dia-
betes (T2D). However, con icting outcomes have been reported.This meta-analysis aimed to predict the association
between the HMGA1 variant IVS5-13insC and T2D. Statistical analyses were performed using Stata/SE 12.0 software.
A total of 11 case-control studies in 6 articles including 18,539 diabetic patients and 18,228 non-diabetic patients
were conducted in Europe, Asia and South America. Results suggested that the HMGA1 variant IVS5-13insC was
associated with an increased risk of insulin resistance (OR = 0.61, 95% CI 0.56 to 0.66, P < 0.0001), T2D (OR = 0.67,
95% CI 0.61 to 0.73, P < 0.0001), particularly for Caucasians with increased risks of T2D (OR = 0.56, 95% CI 0.49
to 0.65, P < 0.0001) compared with wild-type subjects. This meta-analysis indicated that the HMGA1 variant IVS5-
13insC can be a risk factor of T2D development, particularly among Caucasians. Signi cant risks were also found
(Asian: OR = 0.74, 95% CI: 0.63 to 0.86, P < 0.0001, Hispanic-American: OR = 0.81, 95% CI: 0.65 to 1.01, P < 0.0001)
in non-Caucasian population. However, ethnical studies should be conducted to reveal whether the HMGA1 variant
IVS5-13insC is associated with an increased risk of T2D.
KEY WORDS: HMGA1, TYPE 2 DIABETES, INSULIN RESISTANCE, VARIANT, META-ANALYSIS
335
ARTICLE INFORMATION:
*Corresponding Author: wql_zcq@126.com
Received 30
th
Aug, 2016
Accepted after revision 29
th
Sep, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
336 HMGA1 VARIANT IVS5-13INSC IS ASSOCIATED WITH INSULIN RESISTANCE AND TYPE 2 DIABETES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Qinglu Wang et al.
INTRODUCTION
Type 2 diabetes (T2D) is one of the major and exacer-
bating health problems worldwide; T2D is predicted to
affect 490 million in 2030 (Zhang, et al., 2010). Strong
genetic in uences and many polymorphisms have been
reproducibly associated with T2D.Insulin resistance in
muscle, liver, and adipose tissues is a primary charac-
teristic of most patients with T2D; as such, these tissues
become resistant to endogenous and exogenous insulin.
The interaction of insulin with target tissues is mediated
by insulin receptor (INSR), a glycoprotein implicated
in directing insulin to target cells and initiating cell
responses to insulin, (Gold ne, 1987 Herder and Roden,
2011, Voight, et al., 2010).
High-mobility group A1 (HMGA1) is an architectural
transcription factor involved in numerous biological
functions in the nucleus, including regulation of DNA
replication, transcription, recombination, and repair;
among these functions, transcriptional regulation of
gene expression is considered as the most important.
After HMGA1 binds to DNA, HMGA1 can be polymerized
with other transcription factors, forming an “enhanceo-
some” to regulate gene transcription; thus, gene expres-
sions are positively or negatively regulated(Bustin and
Reeves, 1996). Studies on humans and knockout mice
have suggested that HMGA1 is involved in to T2D patho-
genesis through the regulation of INSR gene expres-
sion; INSR gene expression is decreased by functional
HMGA1 gene variants. HMGA1-de cient patients have
been biologically investigated because of their clinical
value. However, whether HMGA1 single gene deletion-
or mutation-induced insulin resistance is the underlying
cause of T2D remains unknown, (Foti, et al., 2005). Low-
frequency insertion polymorphism IVS5-13insC (c.136-
14_136-13insC) has been identi ed and associated with
insulin resistance and T2D among individuals of white
European ancestry and Chinese populations, (Chiefari,
et al., 2011 Liu, et al., 2012).
However, no similar association is observed in another
study involving Caucasians and populations of African
and Hispanic descent. Furthermore, con icting results
regarding the association of HMGA1 with T2D and
insuf cient data on diverse ethnic groups have caused
dif culty in performing clinical translation of HMGA1
IVS5-13insC genotyping, (Marquez et al., 2012, Karnes,
et al., 2013, Pullinger, et al., 2014 ).
Results regarding the functional effect of the HMGA1
IVS5-13insC variant are also contradictory. On the one
hand, HMGA1 and INSR expressions decrease in dia-
betic carriers of IVS5-13insC compared with those of
wild-type diabetic and non-diabetic patients. INSR pro-
tein expression and insulin-binding capacity are also
restored in lymphoblasts obtained from diabetic IVS5-
13insC carriers through HMGA1 DNA transfection,
(Chiefari, et al., 2011).
On the other hand, IVS5-13insC does not affect
HMGA1 or INSR expression in adipose tissues of nor-
moglycemic patients. IVS5-13insC is present at position
13 of HMGA1 exon 6; however, the direct mechanism
by which this variant affects mRNA expression or amino
acid sequence remains unclear, (Marquez, et al., 2012).
A previous meta-analysis of Caucasians focused on
this issue and arrived at a negative conclusion(Marquez,
et al., 2012). Thus, we performed a meta-analysis of eligi-
ble case-control studies worldwide to investigate whether
the HMGA1 variant IVS5-13insC is associated with an
increased risk of insulin resistance and T2D. We also con-
ducted subgroup analyses according to different ethnici-
ties to explore the presence of ethnicity-speci c effects.
MATERIAL AND METHODS
LITERATURE SEARCH STRATEGY
We searched Pubmed, EMBASE, and Web of science.
The last updated search was performed on February 12,
2015. We used any possible combinations of relevant
keywords: “HMGA1 or high-mobility group A1,” “poly-
morphism or mutation or mutant or variant,” and “insu-
lin resistance, T2D, or type 2 diabetes.”
Articles describing the relationship between T2D and
IVS5-13insC were identi ed with no language limi-
tations. The inclusion criteria were set as follows: (a)
evaluation of IVS5-13insC, insulin resistance, and T2D
risk and (b) case-control design to estimate odds ratio
(OR) with a 95% con dence interval (CI). Articles were
excluded according to the following criteria: (a) reviews,
meta-analyses, and other non-case-control studies and
(b) nonhuman studies. For studies with the same or
overlapping data by the same authors, the most suitable
studies with the largest number of cases or latest publi-
cation dates were selected.
DATA EXTRACTION
Two reviewers (Yancheng Liu and Liting Zheng) inde-
pendently extracted information from all of the eligi-
ble publications and reached consensus on all items.
An author (Hao Kong) was invited to assess articles in
cases of disagreement. The following information was
extracted from each article: rst author, journal, year of
publication, country of origin, ethnicity, and exact data
of cases and controls.
STATISTICAL ANALYSIS
The T2D risk associated with IVS5-13insC was evaluated
using ORs with a 95% CI. Heterogeneity (I
2
) was evalu-
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS HMGA1 VARIANT IVS5-13INSC IS ASSOCIATED WITH INSULIN RESISTANCE AND TYPE 2 DIABETES 337
Qinglu Wang et al.
ated using a Cochran’s Q statistic to assess the degree of
inter-study variation. The pooled OR of each study was
calculated using a xed-effects model when no statis-
tically signi cant heterogeneity was detected with a P
value < 0.10. A random-effects model was used when
signi cant heterogeneity was found.
The statistical signi cance of the pooled ORs was
determined using a Z test. P value < 0.05 was consid-
ered signi cant. A strati ed analysis of ethnicity and
continent was also performed: (1) Caucasian and non-
Caucasian and (2) Asian and European. E gger’s plot was
used to evaluate the probability of publication bias. Sta-
tistical analyses were carried out using Stata/SE 12.0 for
Windows.
RESULTS
CHARACTERISTICS OF THE STUDIES
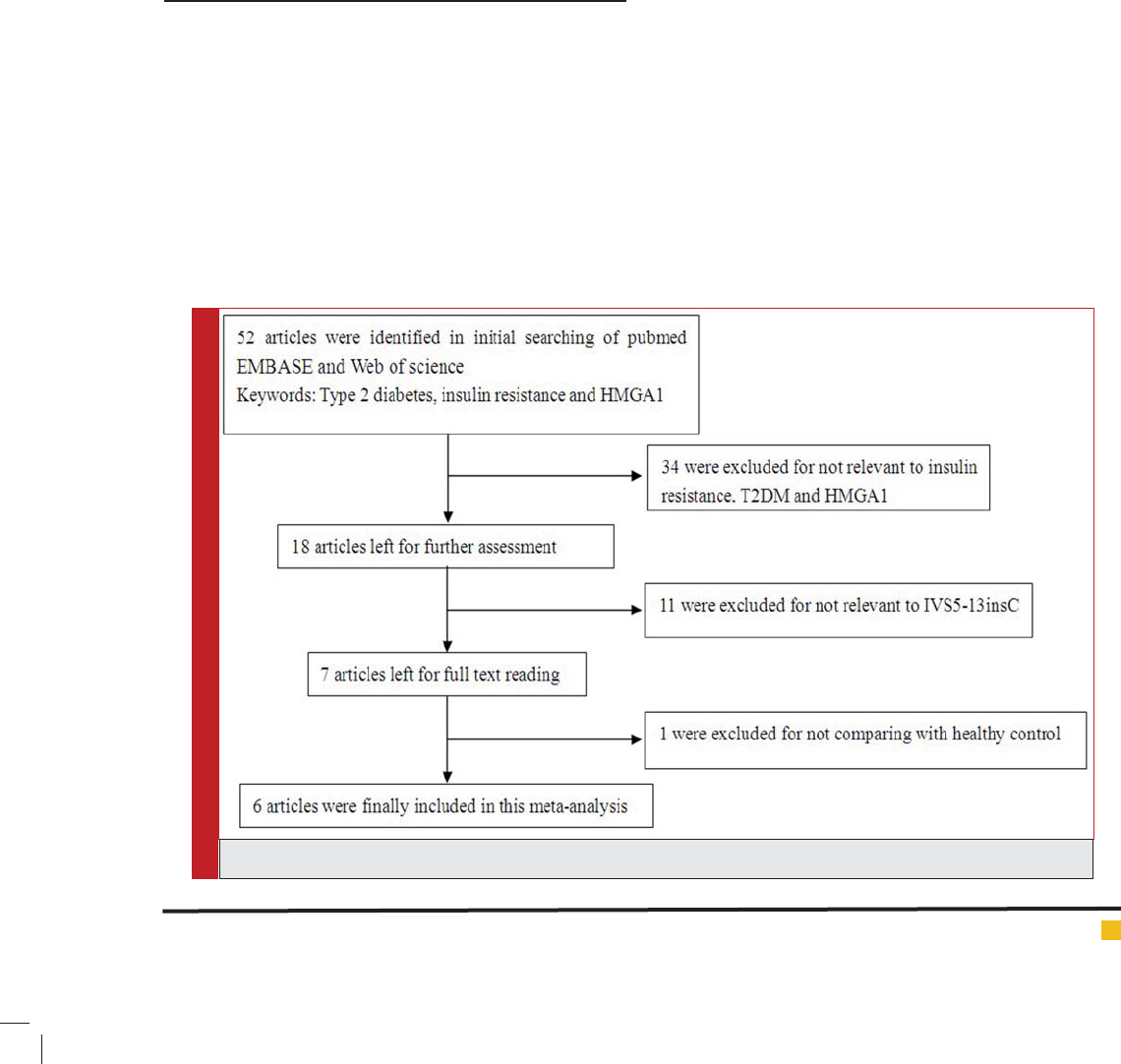
Figure 1 demonstrates the progress of the article selec-
tion. After initially searching PubMed, EMBASE, and
Web of science, we identi ed 52 publications. Of these
52 publications, 34 were excluded after titles and
abstracts were scanned to determine whether or not
these articles are relevant to T2D and HMGA1 polymor-
phism; as a result, 18 articles were considered for fur-
ther assessment. Of these 18 articles, 11 were not related
to the HMGA1 variant IVS5-13insC; thus, these articles
were removed from the list. After reading the full text
of the 7 remaining studies, we excluded 1 article that
did not compare between T2D patients and healthy con-
trols.
As a result, 18,539 diabetic patients and 1 8,228
non-diabetic patients were enrolled to determine the
HMGA1 variant IVS5-13insC. (5 articles about T2D(Liu,
et al., 2012, Chiefari, et al., 2011, Pullinger, et al., 2014,
Karnes, et al., 2013, Marquez, et al., 2012) and 1 article
about MetS(Chiefari, et al., 2013).
The 6 studies included 13,719 diabetic patients and
13,572 non-diabetic patients were came from Europe,
4 studies included 2,112 diabetic patients and 2,081
non-diabetic patients were came from South America,
and 1 study included 2,712 diabetic patients and 2,575
non-diabetic patients were came out of Asia. Thus, 11
case-control studies from 6 articles were included in
our meta-analysis. Reports from other areas were lim-
ited. The detailed information of each study is shown in
Table 1. We estimated the risk between T2D and control
groups by comparing gene frequencies of the HMGA1
variant IVS5-13insC (del/ins, ins/ins) and the wild type
(del/del).
OVERALL META-ANALYSIS AND SUBGROUP
ANALYSIS
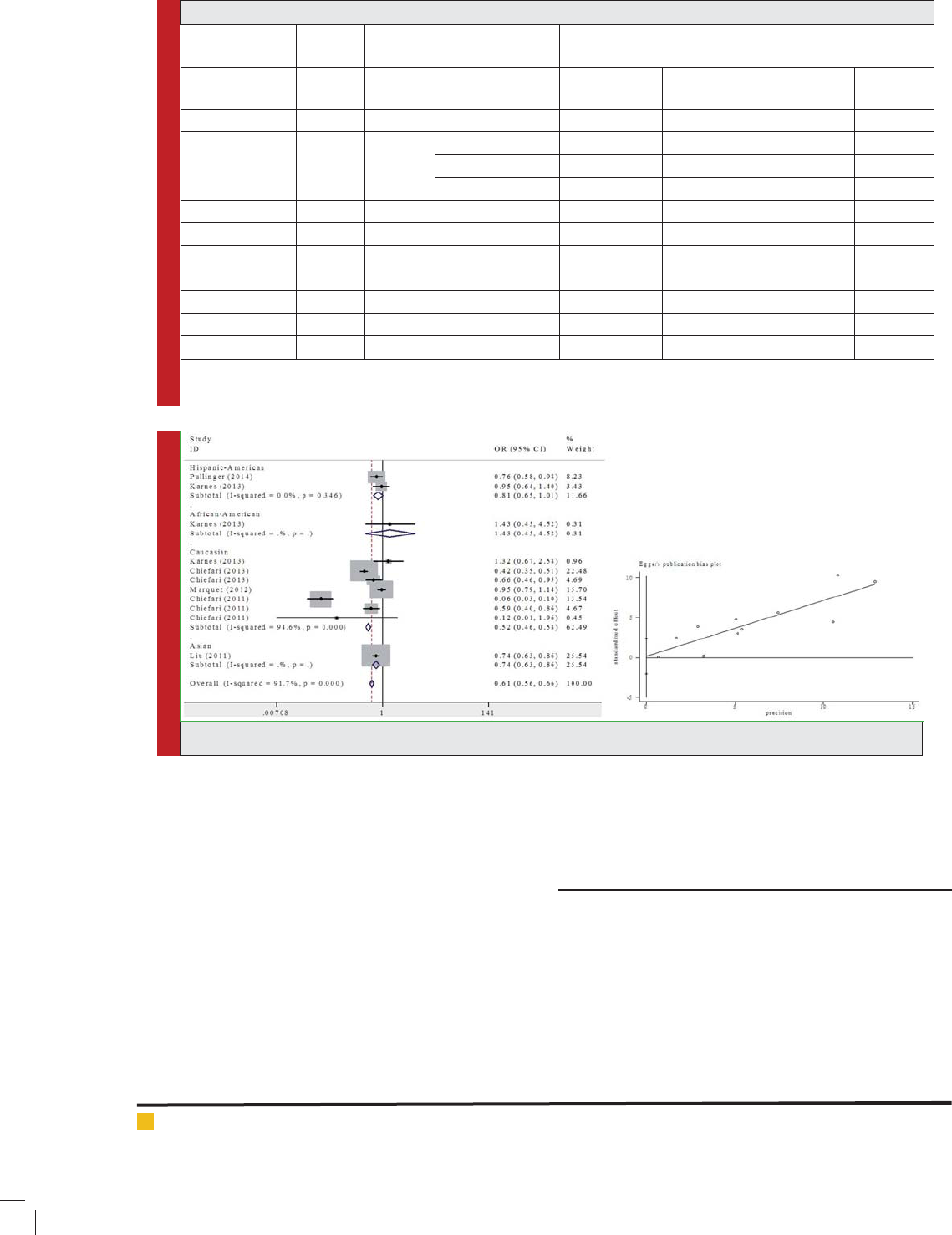
A summary of the meta-analysis of the HMGA1 variant
IVS5-13insC and T2D is shown in Figure 2. The HMGA1
FIGURE 1. Flow diagram of included/excluded studies
338 HMGA1 VARIANT IVS5-13INSC IS ASSOCIATED WITH INSULIN RESISTANCE AND TYPE 2 DIABETES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Qinglu Wang et al.
Table 1: Characteristics of the 11 case-controls included in the meta-analysis
First author
(years)
Disease Country Ethnicity Non-diabetic patients
genotype
Diabetic patients genotype
Mutant type
(c/c or c/-)
Wild type
(-/-)
Mutant type
(c/c or c/-)
Wild type
(-/-)
Pullinger (2014) T2D America Hispanic-American 293 531 135 185
Karnes (2013) T2D America Hispanic-American 45 597 69 868
African-American 6 147 6 210
Caucasian 18 475 17 591
Chiefari (2013) MetS Italian Caucasian 195 4821 299 3106
Chiefari (2013) MetS Turkish Caucasian 57 703 72 587
Liu (2012) T2D China Asian 354 2358 436 2139
Marquez (2012) T2D France Caucasian 228 4159 267 4639
Chiefari (2011) T2D Italy Caucasian 11 2533 237 3041
Chiefari (2011) T2D America Caucasian 45 913 75 895
Chiefari (2011) T2D France Caucasian 0 50 27 327
MetS: The metabolic syndrome is a common multicomponent disorder where insulin resistance is associated with an increased risk
for type 2 diabetes (T2D), hypertension, dyslipidemia, and cardiovascular disease (CVD).
FIGURE 2. Meta-analysis of the HMGA1 variant IVS5-13insC and T2D
variant IVS5-13insC was signi cantly associated with
an increased risk of insulin resistance and T2D com-
pared with that of healthy controls in overall popula-
tions (insulin resistance: OR = 0.61, 95% CI 0.56 to 0.66,
P < 0.0001; T2D: OR = 0.67, 95% CI 0.61 to 0.73, P <
0.0001).
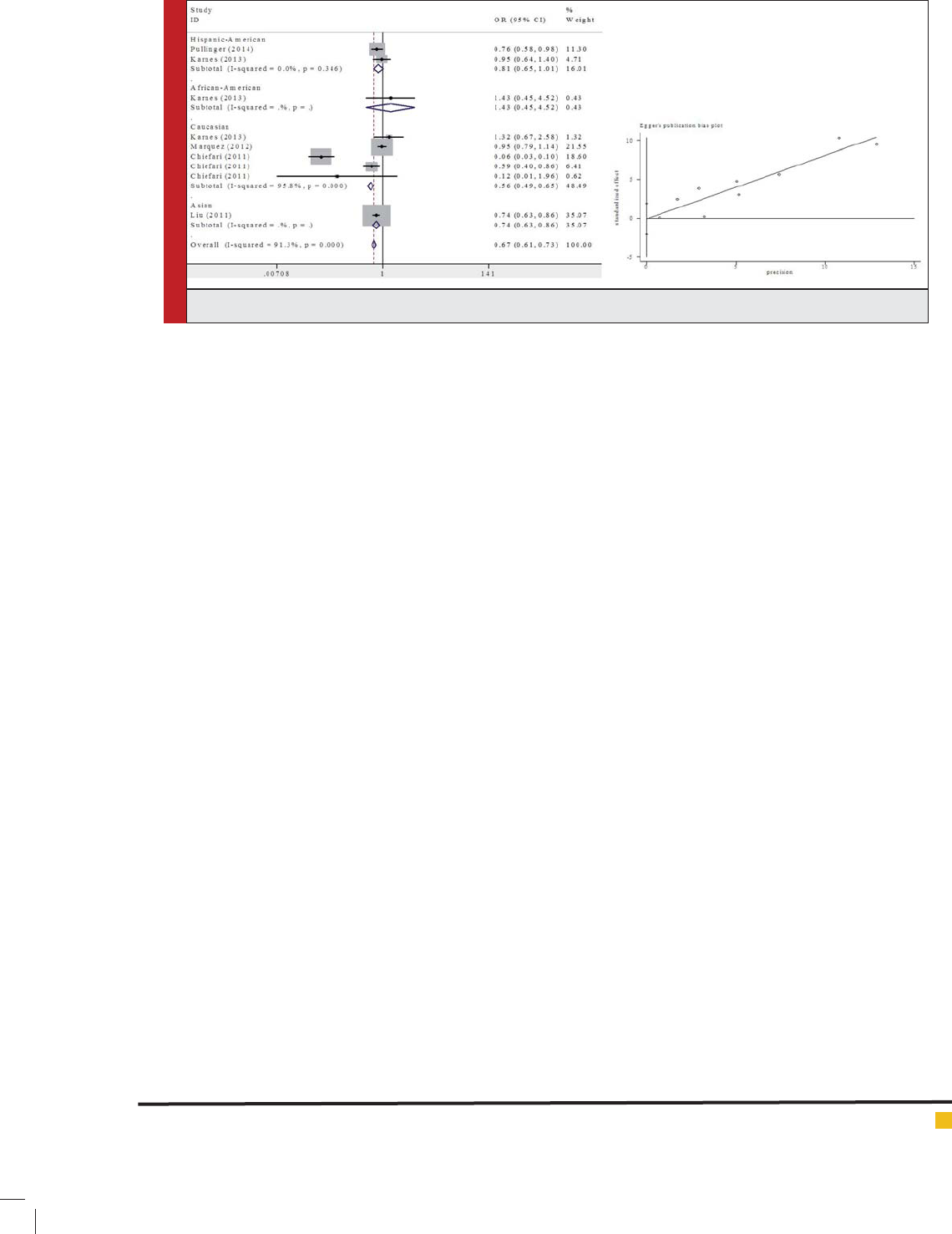
Subgroup analysis was performed according to dif-
ferent ethnic groups in this meta-analysis. Signi cant
associations were found in Figure 3 (OR = 0.56, 95% CI:
0.49 to 0.65, P < 0.0001) in the Caucasian population;
an increasing pattern was observed in non-Caucasian
populations (Asian: OR = 0.74, 95% CI: 0.63 to 0.86, P <
0.0001, Hispanic-American: OR = 0.81, 95% CI: 0.65 to
1.01, P < 0.0001).
Publication bias: Egger’s test revealed a consistent out-
come. Egger’s plot indicated a lack of publication bias.
DISCUSSION
RETROSPECTIVE
This meta-analysis is the rst to identify the increased
T2D vulnerability of the HMGA1 variant IVS5-13insC
variant carriers; our result suggested that the HMGA1
variant IVS5-13insC variant is likely involved in T2D
pathogenesis. However, a previous meta-analysis of
Caucasians revealed that the HMGA1 variant IVS5-
13insC is not associated with T2D. However, our meta-
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS HMGA1 VARIANT IVS5-13INSC IS ASSOCIATED WITH INSULIN RESISTANCE AND TYPE 2 DIABETES 339
Qinglu Wang et al.
analysis of Caucasians and other populations showed
that the HMGA1 variant IVS5-13insC may increase
the prevalence of T2D. Furthermore, the HMGA1 vari-
ant IVS5-13insC may increase the prevalence of T2D in
other ethnic groups.
Genome-wide association studies (GWAS) on patients
with T2D have identi ed associations between polymor-
phisms and mutations in some genes(Hale, et al., 2012).
These genes have been regarded as potential T2D risk
factors. However, current GWAS fail to detect an associ-
ation between the HMGA1 variant IVS5-13insC and the
presence of T2D. To the best of our knowledge, future
meta-analyses that include GWAS datasets will help
determine whether the IVS5-13insC shows a consistent
association with T2D.
LIMITATIONS
The limitations of our study are as follows. First, only
published studies in English were included in our data
analysis; other languages or unpublished materials could
be overlooked. Second, majority of the studies involved
Caucasian populations, whereas four studies focused
on non-Caucasian populations. Thus, further studies on
other populations should be conducted to investigate
such association among non-Caucasian populations.
Third, the ORs obtained using comparison models were
unadjusted; a precise analysis should be conducted if
individual raw data were available. Finally, two meta-
analyses indicated signi cant heterogeneity. Despite
these restrictions, our study provided a comprehensive
understanding of the association between the HMGA1
variant IVS5-13insC and risk of T2D.
CROSS SECTIONAL
In conclusion, the HMGA1 variant IVS5-13insC can
be regarded as a new risk factor of the development of
insulin resistance and T2D, particularly among Cauca-
sians. Furthermore, Asian and Hispanic-American eth-
nic groups fail to indicate ethnic diversity of disease
susceptibility. In the future, case-control investigations
of many ethnic groups and communities should be per-
formed to reveal whether the HMGA1 variant IVS5-
13insC is associated with an increased risk of T2D and
to determine ethnicity-speci c effects.
P ERSPECTIVES
HMGAl plays a crucial role in blood sugar balance as a
structural transcription factor. We believe that an indi-
vidual with the HMGA1 variant IVS5-13insC has clini-
cal implications. First, the presence of these variants
can serve as an early predictive marker of both insu-
lin resistance and T2D, especially for individuals with
family histories of T2D and related conditions. Second,
the presence of these variants may predict responses to
therapy(Smith, et al., 2010). T2D treatment is largely
empirical and the prediction of speci c responses to a
therapeutic agent in any patient is dif cult
10
. Patients
with T2D and variants may respond differently to spe-
ci c therapies, such as an insulin sensitizer, because
HMGA1 variant IVS5-13insC de nes a speci c defect
that decreases insulin receptor concentrations and insu-
lin resistance. Third, individuals possessing functional
HMGA1 variant IVS5-13insC and T2D may have dif-
ferent clinical courses from other patients with T2D,
including differences in the development of compli-
cations. Fourth, the search for new therapies for T2D
can include agents that upregulate HMGA1 expression.
Finally, this conclusion provides some theoretical basis
for HMGA1 single gene deletion- or mutation-induced
insulin resistance as the underlying cause of T2D. Fur-
thermore, IVS5-13insC can be regarded as a novel target
of gene therapy for T2D and insulin resistance.
FIGURE 3. Subgroup meta-analysis of different ethnic groups
340 HMGA1 VARIANT IVS5-13INSC IS ASSOCIATED WITH INSULIN RESISTANCE AND TYPE 2 DIABETES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
The exact biological mechanism underlying the
association between the HMGA1 gene and risk of T2D
remains uncertain. Functional studies and succeeding
replications of these associations are necessary to de ne
the potential role of the HMGA1 variant IVS5-13insC
in predicting T2D developments. Although the cur-
rent study provides this conclusion, further studies on
HMGA1 are warranted to clarify the role of this gene in
diabetes pathogenesis.
HMGA1 has been extensively investigated. HMGA1
is highly expressed in tumor cells; furthermore, HMGA1
is implicated in tumor initiation and progression by
disrupting the stability of mitochondrial genome or
by participating in the transcriptional regulation of
gene expression related to tumors(Mao, et al., 2009).
Thus, accurate physiological characteristics of HMGA1
polymorphism should be determined through several
approaches.
DECLARATION OF INTEREST
We declare that there no any nancial or other potential
con ict of interest, and there is no con ict of interest
that could be perceived as prejudicing the impartiality
of the research reported.
ACKNOWLEDGMENTS
This work was supported by grants from the Natural
Scienti c Foundation of Shandong Province, China
(ZR2014CM046, ZR2010CQ031 and ZR2015CL019) and
Collaborative Innovation Center of Chinese medicine
antivirus in Shandong University of Tranditional Chi-
nese Medicine (XTCX2014B01-07).
REFERENCES
Bustin M and R. Reeves (1996): High-mobility-group chromo-
somal proteins: architectural components that facilitate chro-
matin function. Prog Nucleic Acid Res Mol Biol, 54, 35-100
Chiefari E, S. Tanyolac, S. Iiritano, A. Sciacqua, C. Capula, B.
Arcidiacono, A. Nocera, K. Possidente, F. Baudi, V. Ventura, G.
Brunetti, F. S. Brunetti, R. Vero, R. Maio, M. Greco, M. Pavia,
U. Hodoglugil, V. Durlach, C. R. Pullinger, I. D. Gold ne, F.
Perticone, D. Foti and A. Brunetti (2013): A polymorphism of
HMGA1 is associated with increased risk of metabolic syn-
drome and related components. Sci Rep, 3, 1491
Chiefari, E., S. Tanyolac, F. Paonessa, C. R. Pullinger, C. Capula,
S. Iiritano, T. Mazza, M. Forlin, A. Fusco, V. Durlach, A. Dur-
lach, M. J. Malloy, J. P. Kane, S. W. Heiner, M. Filocamo, D. P.
Foti, I. D. Gold ne and A. Brunetti (2011): Functional variants
of the HMGA1 gene and type 2 diabetes mellitus. JAMA, 305,
903-912
Foti, D., E. Chiefari, M. Fedele, R. Iuliano, L. Brunetti, F. Paon-
essa, G. Man oletti, F. Barbetti, A. Brunetti, C. M. Croce and A.
Fusco (2005): Lack of the architectural factor HMGA1 causes
insulin resistance and diabetes in humans and mice. Nat Med,
11, 765-773
Gold ne ID (1987): The insulin receptor: molecular biology
and transmembrane signaling. Endocr Rev, 8, 235-255
Hale PJ , A. M. Lopez-Yunez and J. Y. Chen (2012): Genome-
wide meta-analysis of genetic susceptible genes for Type 2
Diabetes. BMC Syst Biol, 6 Suppl 3, S16
Herder H., and M. Roden (2011): Genetics of type 2 diabetes:
pathophysiologic and clinical relevance. Eur J Clin Invest, 41,
679-692
Karnes JH, T. Y. Langaee, C. W. McDonough, S. W. Chang, M.
Ramos, J. R. Catlin, Jr., O. E. Casanova, Y. Gong, C. J. Pepine, J.
A. Johnson and R. M. Cooper-Dehoff (2013): Lack of associa-
tion of the HMGA1 IVS5-13insC variant with type 2 diabetes
in an ethnically diverse hypertensive case control cohort. J
Transl Med, 11, 12
Liu, L., H. Ding, H. R. Wang, Y. J. Xu, G. L. Cui, P. H. Wang,
G. Yuan, X. F. Yu and D. W. Wang (2012): Polymorphism of
HMGA1 is associated with increased risk of type 2 diabetes
among Chinese individuals. Diabetologia, 55, 1685-1688
Mao M, K. J. Wertzler, S. C. Maloney, Z. Wang, N. S. Magnuson
and R. Reeves (2009): HMGA1 levels in uence mitochondrial
function and mitochondrial DNA repair ef ciency. Mol Cell
Biol, 29, 5426-5440
Marquez M, M. Huyvaert, J. R. Perry, R. D. Pearson, M. Fal-
chi, A. P. Morris, S. Vivequin, S. Lobbens, L. Yengo, S. Gaget,
F. Pattou, O. Poulain-Godefroy, G. Charpentier, L. M. Carls-
son, P. Jacobson, L. Sjostrom, O. Lantieri, B. Heude, A. Walley,
B. Balkau, M. Marre, P. Froguel and S. Cauchi (2012): Low-
frequency variants in HMGA1 are not associated with type 2
diabetes risk. Diabetes, 61, 524-530
Pullinger CR, I. D. Gold ne, S. Tanyolac, I. Movsesyan, M.
Faynboym, V. Durlach, E. Chiefari, D. P. Foti, P. H. Frost, M.
J. Malloy, A. Brunetti and J. P. Kane (2014): Evidence that an
HMGA1 gene variant associates with type 2 diabetes, body
mass index, and high-density lipoprotein cholesterol in a
Hispanic-American population. Metab Syndr Relat Disord, 12,
25-30
Smith RJ, D. M. Nathan, S. A. Arslanian, L. Groop, R. A. Rizza
and J. I. Rotter (2010): Individualizing therapies in type 2 dia-
betes mellitus based on patient characteristics: what we know
and what we need to know. J Clin Endocrinol Metab, 95, 1566-
1574
Voight BF., L. J. Scott, V. Steinthorsdottir, A. P. Morris, et al.,
(2010): Twelve type 2 diabetes susceptibility loci identi ed
through large-scale association analysis. Nat Genet, 42, 579-
589
Zhang,P X. Zhang, J. Brown, D. Vistisen, R. Sicree, J. Shaw
and G. Nichols (2010): Global healthcare expenditure on dia-
betes for 2010 and 2030. Diabetes Res Clin Pract, 87, 293-301
Qinglu Wang et al.