
Medical
Communication
Biosci. Biotech. Res. Comm. 9(3): 553-557 (2016)
Association of hypo ferritinemia and restless legs
syndrome in patients with iron de ciency anemia
M. Abbasi,
1
B. Safarzadehkhoushabi
1*
and M S. Rabiei
2
1
Department of Hematology, Hamadan University of Medical Sciences, Hamadan, Iran
2
Department of Community Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
ABSTRACT
Restless legs syndrome (RLS) is one of the sleep disorders which affects sleep stages and causes repetitive awaken-
ings. The patho physiology of RLS is not well de ned, but there are some evidences about the role of iron de ciency
in these patients. Therefore, in the current research we investigated the frequency of iron de ciency anemia in such
cases. 143 patients referred to Hamedan University of Medical Sciences associated Hospital within the year 2015 with
hypoferritinemia underwent a cross sectional study. All collected data were classi ed and analyzed by SPSS 16; t-test
and chi-square tests. Of the 143 hypoferritinemic patients; 39 patients (27.3 %) met RLS criteria. Of that 17 cases
(43.58 %) were male and 22 persons (56.41 %) were female. According to the study restless legs syndrome was signi -
cantly more common in women than men.(P-value = 0.01). Restless legs syndrome was signi cantly associated with
serum ferritin levels in both sexes. And serum ferritin was signi cantly lower in men and women with non-infected
people. (P-value <0.01). RLS was signi cantly more common in females than males. RLS was signi cantly higher in
low ferritin levels. On the other hand its relation with low serum ferritin in both males and females is signi cant.
KEY WORDS: RESTLESS LEGS SYNDROME, HYPOFERRITINEMIA, IRON, ANEMIA
553
ARTICLE INFORMATION:
*Corresponding Author: Babak Safarzadehkhoushabi thesis.
irani@gmail.com
Received 29
th
Aug, 2016
Accepted after revision 30
th
Sep, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
INTRODUCTION
Restless legs syndrome is a sleep disorder, including
periodic limb movements in sleep (PLMS). A condition
that occurs voluntary movements of limbs during sleep
cycle and alters the level (stage) of sleep and waking
are consecutive. Restless legs syndrome can be divided
into two types: type of family (primary) with known
genetic component, and acquired (secondary). Primary
type is seen in about fty percent of rst-degree rela-
tives of patients and believed to have a hereditary defect
in the metabolism of dopamine.Acquired type includes
changes in the metabolism of iron in a range of patients,
including pregnant women, and people with end stage
554 HYPO FERRITINEMIA AND RESTLESS LEGS SYNDROME WITH IRON DEFICIENCY ANEMIA BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Abbasi, Safarzadehkhoushabi and Rabiei
renal disease patients with iron de ciency and patients
with Vitamin B12 de ciency. Periodic limb movements
in sleep, such as restless legs syndrome may also occur
in a situation such as Parkinson, Narcolepsy and other
diseases with impaired dopamine production. The nega-
tive impact on quality of life is equal to or greater than
chronic obstructive pulmonary disease or myocardial
infarction. Severe restless legs syndrome causes the high-
est levels of sleep deprivation, among all sleep disorders
after mania, (Trenkwalder,1996, Montplaisir 2000,Allen,
2001 Mehmood et al., 2014 and Minár et al 2015).
The prevalence of PLMS is higher in the elderly. Max-
imally thirty percent of people over fty years’ expe-
rience the disease secondary to an underlying medical
condition or drug side effects Restless legs syndrome is
more common among elderly people and about ten to
twenty percent of people over sixty- ve years’ experi-
ence the symptoms more speci cally. The prevalence of
the disease in women is doubled, (Ohayon,2000, Roth-
dach, 2000 Allen,2003). Studies in North America and
northern Europe also con rm that the prevalence of rest-
less legs syndrome (between ve to twenty- ve percent
of the population) is common disease, (Zucconi,2004).
The population whom are at risk for restless legs
syndrome include: pregnant women, patients with end-
stage renal disease, patients with a positive family his-
tory, patients with iron de ciency anemia, frequent
blood donors, patients undergoing stomach surgery and
children with hyperactivity syndrome- decreased atten-
tion and vitamin B12 de ciency. It seems characteris-
tic feature of restless legs syndrome, is associated with
circadian functional elements dopamine pathway. The
circadian pattern of blood iron level is such that on the
night, fty to sixty percent below the level of serum
iron in comparison to day. Patients prone to iron de -
ciency, have a greater chance of developing restless legs
syndrome. These groups included patients undergoing
gastric bypass surgery continuous blood donors as well
as elderly, (Banerji, 1970, Tarquini,1978, O’Keeffer,1994,
Hagan 1999, Silber, 2003, Borreguero, 2004, Earley,
2005 and Gamaldo, 2006 and Çurgunlu et al., 2012).
Restless Legs Syndrome also includes spontaneous or
voluntary movement like walk, shrug, wrong handling
or rubbing the legs on the bed for loss of sensation such
as tingling, itching, burning, heave or electric shock is
felt. Symptoms of this syndrome are the circadian pat-
tern. So in the morning and evening worsen. About
twenty percent of people with restless legs syndrome
have no voluntary movements during sleep (therefore
not required to identify). Although it causes severe sleep
disturbance in most patients, and is known as one of the
causes of sleep de cit in ve to ten percent of Ameri-
cans. Although restless legs syndrome is a common neu-
rological motor disorder but under diagnosed and under
treated in many cases. On the other hand, due to lack of
awareness of health staff about the syndrome, diagnosis
and treatment of this syndrome is commonly missed,
(Walters, 1995, Hening 2004 Wilson, 2005 and Curgunlu
et al., 2012).
Researches on the prevalence of restless legs syn-
drome is not well established. The proper treat-
ment of this syndrome needs recognizing the extent
of it. Therefore it is concerned, Investigations about
the prevalence of this syndrome, the age and sex
of distribution in the society seems to be effective.
The recognition of this disease by the medical staff will
save the patients from ineffective treatments and some-
times misplaced and can take a step towards improving
the quality of life in these patients.
MATERIAL AND METHODS
This study was cross sectional research which was con-
ducted on patients with Hypoferritinemia, referring to
Hamedan University of medical sciences associated Hos-
pital in 2015. Inclusion criteria included: willingness to
participate in the study, ferritin less than 50 mg per dL
for women and less than 100 milligrams per deciliter for
men.
Exclusion criteria included: impairment of conscious-
ness (inability to respond to questions), physical-mental
disability (inability to work with the researcher), drug
addiction, current pregnancy (prone to anemia), sodium
valproate or carbamazepine or gabapentin or hypnotic
drugs (suppression of the symptoms of restless leg syn-
drome), Parkinson’s disease (mimic symptoms of restless
leg syndrome), history of renal failure (risk of anemia )
and a history of gastric surgery (gastric bypass) (prone
to anemia), diabetes mellitus ( symptoms of neuropa-
thy), history of diseases that can be seen in the process
of neuropathy) malabsorption syndrome, a de ciency of
vitamin B, Lyme disease, AIDS, cancer, malignancies of
the blood system and reticuloendothelial).
Questionnaire Form which was used in this
study, consisted of two parts. The rst part included
demographic information, including age, sex
and place of residence (urban/rural), respectively.
The second part of the questionnaire included ve ques-
tions, the patient was asked by the researcher. All of these
questions had yes or no answer and if rst 4 questions
answered (Yes) the diagnosis of restless legs syndrome
was made for the individual. The last question was about
the family history of the disease in her/his family. Some
of the patients participating in the study refused. The
numbers of patients providing inaccurate information
were prevented from doing the proper research. To solve
this problem, researchers questioned more patients to
achieve the desired volume. The reliability and accuracy
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS HYPO FERRITINEMIA AND RESTLESS LEGS SYNDROME WITH IRON DEFICIENCY ANEMIA 555
Abbasi, Safarzadehkhoushabi and Rabiei
was assessed during questioning meaning that patients
with or without the necessary accuracy in speech, not
included in this study.
Values were presented as Mean ±Standard deviation
(SD). For statistical analysis, SPSS software (Version 16,
Chicago, IL, USA) was used applying chi
2
and T test. P
< 0.05 was de ned as signi cant.The study population
voluntarily participated in the investigation. Verbal con-
sent was obtained from the participants for publication
of the research results.
RESULTS AND DISCUSSION
In this study, 143 patients referred to the clinic of Hamedan
hospital in 2015 that do not qualify for exclusion criteria
and met the inclusion criteria for the study were involved.
Of these, 102 (71.3%) women and 41 (28.7%) were male.
(Table 1,2,3,4)
The average age of women participating in the study
was 34.35±9.9 years and mean age was 45.8± 9.0 for
men. Based on the ndings of a CBC among the par-
ticipants, 12 patients (8.4%) had iron de ciency anemia
and 131 (91.6%) did not have iron de ciency anemia.
The mean serum ferritin for women participated in the
project was 35.87±9.4 mg per deciliter and for men was
64.0±21.0 mg per deciliter.
According to the study, 39 cases (27.3%) of
patients with low ferritin diagnosed with restless legs
syndrome And 104 (72.7%) cases did not express
symptoms of this syndrome. The mean serum fer-
ritin level in patients was 29.33±9.9 mg per decili-
ter versus 49.43±18.34 mg per dL in healthy cases.
The average age of men suffering from this syndrome
was 54±6.12 years and in females was 45.045±5.5. Serum
Ferritin level was 40.11±2.2 mg per deciliter in men with
this syndrome and this amount was 21± 2.5 for women.
Moreover, 7 cases (17.9%) of the patients had a positive
family history for this syndrome. And 32 (82.1%) had
no family history. In contrast, 104 (72.72%) of patients
with low ferritin levels were not affected by restless legs
syndrome. Of these, 80 patients (76.92%) were women
and 24 (23.07%) were male, (Table 2,3,4).
According to the study restless legs syndrome was
signi cantly more common in women than men.
(P-value = 0.01).In this study, it was con rmed that
restless legs syndrome is not associated with iron de -
ciency anemia signi cantly. (P-value = 0.24). Accord-
ing to the study restless legs syndrome was signi -
cantly associated with serum ferritin levels in both
sexes. And serum ferritin was signi cantly lower in men
and women with non-infected people. (P-value <0.01)
Ferritin levels in women with this syndrome was asso-
ciated, signi cantly (P-value <0.01), but the men were
not able to determine the signi cance of the data.
In this study, positive family history of the syn-
drome did not approved. (P-value = 0.75)
Restless legs syndrome in both sexes were also signi -
cantly associated with age and was more common in
older age. (P-value <0.01).
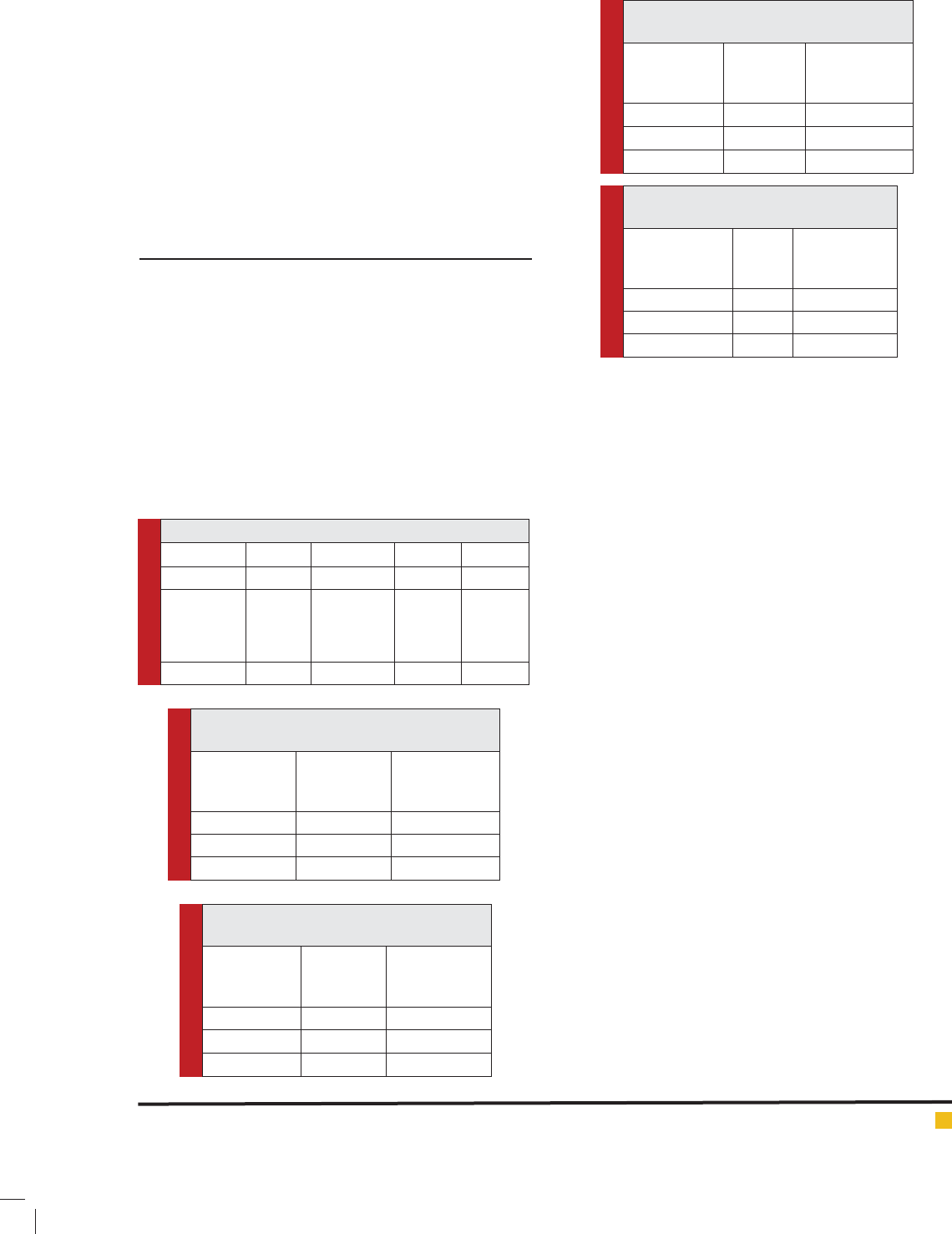
Table 1: The distribution of cases in this series
Male percent female percent total
17 43.6 22 56.4 39(100%)
Low ferritin
with iron
de ciency
anemia
Low ferritin
without iron
de ciency
anemia
5 12.8 34 87.2 39(100%)
Table 2: Frequency of restless legs syndrome
in females based on ferritin levels
Serum
ferritin level
Total
females
restless legs
syndrome
cases
0-15 0 0
15-30 22 22
30-50 80 0
Table 3: Frequency of restless legs
syndrome in males based on ferritin levels
Serum
ferritin level
Total
males
restless legs
syndrome
cases
0-15 1 0
15-30 29 7
30-50 11 10
Table 4: Frequency of restless legs
syndrome in females based on age groups
Serum
ferritin level
Total
females
restless legs
syndrome
cases
0-30 42 0
30-50 50 18
More than 50 10 4
Table 5: Frequency of restless legs
syndrome in males based on age groups
Serum ferritin
level
Total
males
restless legs
syndrome
cases
0-30 0 0
30-50 0 0
More than 50 41 17

556 HYPO FERRITINEMIA AND RESTLESS LEGS SYNDROME WITH IRON DEFICIENCY ANEMIA BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Abbasi, Safarzadehkhoushabi and Rabiei
According to the ndings of our research it was found
that restless legs syndrome was signi cantly seen in
lower levels of ferritin. The syndrome is more common
in women but not signi cantly correlated with anemia.
Çurgunlu and colleagues in Turkey in 2012 reported that
the restless legs syndrome in patients with low ferritin
level was more frequent, (Çurgunlu et al., 2012).
Restless legs Syndrome (RLS) is a kind of sleep disor-
ders; disturbing sleep stages and causes repetitive awak-
ens. High risk populations for RLS including: pregnant
ladies, end stage renal disease patients, patients with
familial history for that, patients with iron de ciency
anemia, chronic blood donors and patients with gastric
bypass surgery and kids with ADHD and people with
vitamin B12 de ciency. The diagnosis of RLS consists of
four essential clinical criteria based solely on symptoms:
A sensation of an urge to move the limbs (commonly
legs); is usually associated with paresthesia. Onset or
worsening of symptoms when at rest; are not associated
with any speci c body position. Relief of symptoms with
movement; complete relief immediately or shortly after
initiating movement was also seen. Marked circadian
variation in degree or occurrence of symptoms; worse in
the evening, got improved in the morning, regardless of
quality or quantity of sleep.
Although Hogl and colleagues in 2005, did not reveal
any relationship between levels of serum ferritin; and
transferrin levels in serum, levels of free iron and restless
legs syndrome, however, stated that the soluble trans-
ferrin receptor (sTR) was signi cantly lower in patients
with this syndrome. In this study, high levels of serum
sTR was independent predictor of the risk of restless legs
syndrome, (Hogl, 2005).
This study, like those of Rothdach et al (2000), Ohayon
et al (2002) and Zucconi et al (2004), presently reports
that the syndrome is more common in older ages, which
is similar to the above ndings. Bjorvatn and colleagues
in a study in 2005 have also found that the age wise
prevalence of this syndrome existed in two Scandina-
vian countries, being in cases of older than 30 years, on
the other hand, there were no signi cant relationships
with age as reported by Bjorvatn et al., (2005).
In this study, 17.9% of the participants had a positive
family history for this syndrome. Although this percent-
age is about 40-60% which was reported by Zucconi et
al, (2004) but a signi cant relationship was not found
in our study. That’s probably due to lack of recognition
of this syndrome in the past by the public and health
professionals (Zucconi 2004). Çurgunlu et al., have
stated that the prevalence of this syndrome in women
is two times more than men. This nding has also been
con rmed by Ohayon (2002) and Zucconi, (2004). In
our study, the relationship between restless legs syn-
drome and serum ferritin was observed. Although more
studies are needed to con rm or refuse this theory.
In a study conducted by Blake et al. (1976), it has been
reported that iron is required for the production of tyros-
ine hydroxylase which is the limiting step in the produc-
tion. Some recent workers have reported that patients
who had serious symptoms of restless leg syndrome, got
it declined by supplements of iron, (Connor, et al., 2003,
Mehmood et al., 2014 and Minár et al 2015). Likewise,
we also report in this paper that serum iron level distur-
bances play a signi cant role in the pathophysiology of
restless legs syndrome.
CONCLUSION
Finally, this study concluded that the frequency of restless
legs syndrome in patients with low ferritin is about 27.3%.
This syndrome was signi cantly associated with reduced
levels of serum ferritin. Also this syndrome in elderly and
especially in women is more prevalent. Further studies
with larger sample size and prospective in urban and rural
centers, specialized treatment centers needs to be done. It
is suggested based on the ndings of this study, subjects
with low serum ferritin, even without laboratory ndings
of anemia, to improve the quality of sleep, or prevent the
syndrome can be treated with oral iron supplements.
REFERENCES
Allen RP, Earley CJ.(2001) Restless legs syndrome: a review
of clinical and pathophysiologic features. J Clin Neurophys-
iol;18:128-147.
Allen RP, Picchietti D, Hening WA.( 2003) Restless legs syn-
drome: diagnostic criteria, special considerations, and epide-
miology. A report from the restless legs syndrome diagno-
sis and epidemiology workshop at the National Institutes of
Health. Sleep Med;4:101-119.
Banerji N, Hurwitz LJ. (1970) Restless legs syndrome, with par-
ticular reference to its occurrence after gastric surgery. Br Med
J;4:774-775.
Blake DR, Williams AC, Pall H.(1986) Iron and akathisia. Br
Med J;292:1393.
Bjorvatn B, Leissner L, Ulfberg J. (2005) Prevalence, severity
and risk factors of restless legs syndrome in the general adult
population in two Scandinavian countries. Sleep Med;6:307-
312.
Connor JR, Boyer PJ, Menzies SL.(2003) Neuropathological
examination suggests impaired brain iron acquisition in rest-
less legs syndrome. Neurology;61:304-309.
Çurgunlu A, Döventas A, Karadeniz D, Erdinçler DS, Oztürk
AK, Karter Y,Yaldiran A, Sipahioglu F, Beger T.(2012) Preva-
lence and characteristics of restless legs syndrome (RLS) in the
elderly and the relation of serum ferritin levels with disease
severity: hospital-based study from Istanbul, Turkey. Arch
Gerontol Geriatr; 55:73-76.

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS HYPO FERRITINEMIA AND RESTLESS LEGS SYNDROME WITH IRON DEFICIENCY ANEMIA 557
Abbasi, Safarzadehkhoushabi and Rabiei
Earley CJ, Connor JR, Beard JL.(2005) Ferritin levels in the cer-
ebrospinal uid and restless legs syndrome: effects of different
clinical phenotypes. Sleep;28:1069-1075.
Gamaldo CE, Earley CJ.(2006) Restless legs syndrome: a clini-
cal update. Chest;130:1596-1604.
Garcia-Borreguero D, Serrano C, Larrosa O, Granizo JJ.(2004)
Circadian effects of dopaminergic treatment in restless legs
syndrome. Sleep Med;5:413-420.
Hagan MM, Havel PJ, Seeley RJ.(1999) Cerebrospinal uid and
plasma leptin measurements: covariability with dopamine and
cortisol in fasting humans. J Clin Endocrinol Metab;84:3579-
3585.
Hening W, Walter AS, Allen RP. (2004) Impact, diagnosis and
treatment of restless legs syndrome (RLS) in a primary care
population: the REST (RLS epidemiology, symptoms, and treat-
ment) primary care study. Sleep Med;5:237-246.
Hogl B, Kiechl S, Willeit J. (2005)Restless legs syndrome: a
community-based study of prevalence, severity, and risk fac-
tors. Neurology;64:1920-1924.
Mehmood T, Auerbach M, Earley CJ, Allen RP.(2014) Response
to intravenous iron in patients with iron de ciency anemia
(IDA) and restless leg syndrome (Willis-Ekbom disease). Sleep
Med.;15(12):1473-6. doi: 10.1016/j.sleep.2014.08.012.
Minár M, Košutzká Z, Habánová H, Rusnák I, Planck K,
Valkovic P.(2015) Restless legs syndrome in pregnancy is
connected with iron de ciency. Sleep Med.;16(5):589-92.
doi: 10.1016
Montplaisir J, Michaud M, Denesle R, Gosselin A.(2000) Peri-
odic leg movements are not more prevalent in insomnia or
hypersomnia but are speci cally associated with sleep disor-
ders involving a dopaminergic impairment. Sleep Med;1:163-
167.
Ohayon MM, Roth T. (2000) Prevalence of restless legs syn-
drome and periodic limb movement disorder in the general
population. J Psychosom Res;53:547-554.
O’Keeffe ST, Gavin K, Lavan JN.(1994) Iron status and the
restless legs syndrome in the elderly. Age Ageing;23:200-
203.
Rothdach AJ, Trenkwalder C, Haberstock J.(2000) Prevalence
and risk factors of RLS in an elderly population: the MEMO
study. Memory and Morbidity in Augsburg Elderly. Neurol-
ogy;54:1064-1068.
Silber MH, Richardson JW.(2003) Multiple blood donations
associated with iron de ciency in patients with restless legs
syndrome. Mayo Clin Proc;78:52-54.
Tarquini B.(1978) Iron metabolism: clinical chronobiological
aspects. Chronobiologia;5:315-336.
Trenkwalder C, Seidel VC, Gasser T, Oertel WH.(1996) Clini-
cal symptoms and possible anticipation in a large kindred of
familial restless legs syndrome. Mov Disord;11:389-394.
Walters AS.( 1995) Toward a better de nition of restless legs
syndrome. The International Restless Legs Syndrome Study
Group. Mov Disord;10:634-642.
Wilson JF. (2005) Is sleep the new vital sign? Ann Intern
Med;142:877-880.
Zucconi M, Ferini-Strambi L.(2004) Epidemiology and clini-
cal ndings of restless legs syndrome. Sleep Med;5:293-
299.