
Medical
Communication
Biosci. Biotech. Res. Comm. 9(3): 366-370 (2016)
Deposition of monomeric C-reactive protein as
evidence of localised neurodegenerative diseases
Al Hsinawi M
1
and Al Baradie R*
2
1
King Khaled Majmaah Hospital, Al Majmaah, Kingdom of Saudi Arabia
2
Medical Laboratories Department, College of Applied Medical Sciences, Majmaah University, Al Majmaah,
Malek M Al-Hsinawi Director, King Khaled Majmaah Hospital Al Majmaah Kingdom of Saudi Arabia
Kingdom of Saudi Arabia
ABSTRACT
Monomeric-C-reactive protein (mCRP) is deposited in signi cant quantities within the brain parenchyma after stroke.
Since we have recently identi ed a possible role of this protein in supporting neurodegeneration and aberrant vascu-
lar development, we identi ed a small group of post-mortem brain samples from individuals who had AD and on his-
tological examination, evidence of tissue infarction/micro-infarction. Here we show that mCRP deposition is highest
in those regions affected by stroke or vascular disruption, and that within those same areas, there is more interaction
and co-localization between major classical proteins of neurodegeneration (-amyloid and tau. We hypothesise that
vascular disruption and concomitant release of mCRP within the brain tissue could exacerbate ongoing neurologi-
cal damage via stimulation of neuro-in ammation and from direct consequences of its action on both neuronal and
vascular health.
KEY WORDS: MONOMERIC C-REACTIVE PROTEIN; STROKE; ALZHEIMER’S DISEASE; NEURODEGENERATION; VASCULAR DEMENTIA
366
ARTICLE INFORMATION:
*Corresponding Author: raid5555@hotmail.com
Received 1
st
Sep, 2016
Accepted after revision 30
th
Sep, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
INTRODUCTION
We have shown previously that monomeric C-reactive
protein (mCRP) was dramatically over-expressed in the
brain extracellular matrix (ECM) of patients following
acute ischaemic stroke (Slevin, 2010). In addition, mCRP,
unlike the native pentameric molecule (pCRP), stimulated
aberrant angiogenesis in vitro, induced phosphorylation
of Tau by neurons and Tau-244-372 aggregation in vitro
and following injection into the hippocampus of mice,
directly resulted in cognitive and memory decline simi-
lar to that seen in a model of Alzheimer’s disease (AD)
(Tg x 3) ( Slevin, 2015).
mCRP also has been co-localised with CD105 in
microvessels suggesting angiogenesis. Phospho-arrays/
Western blotting identi ed signalling activation in both
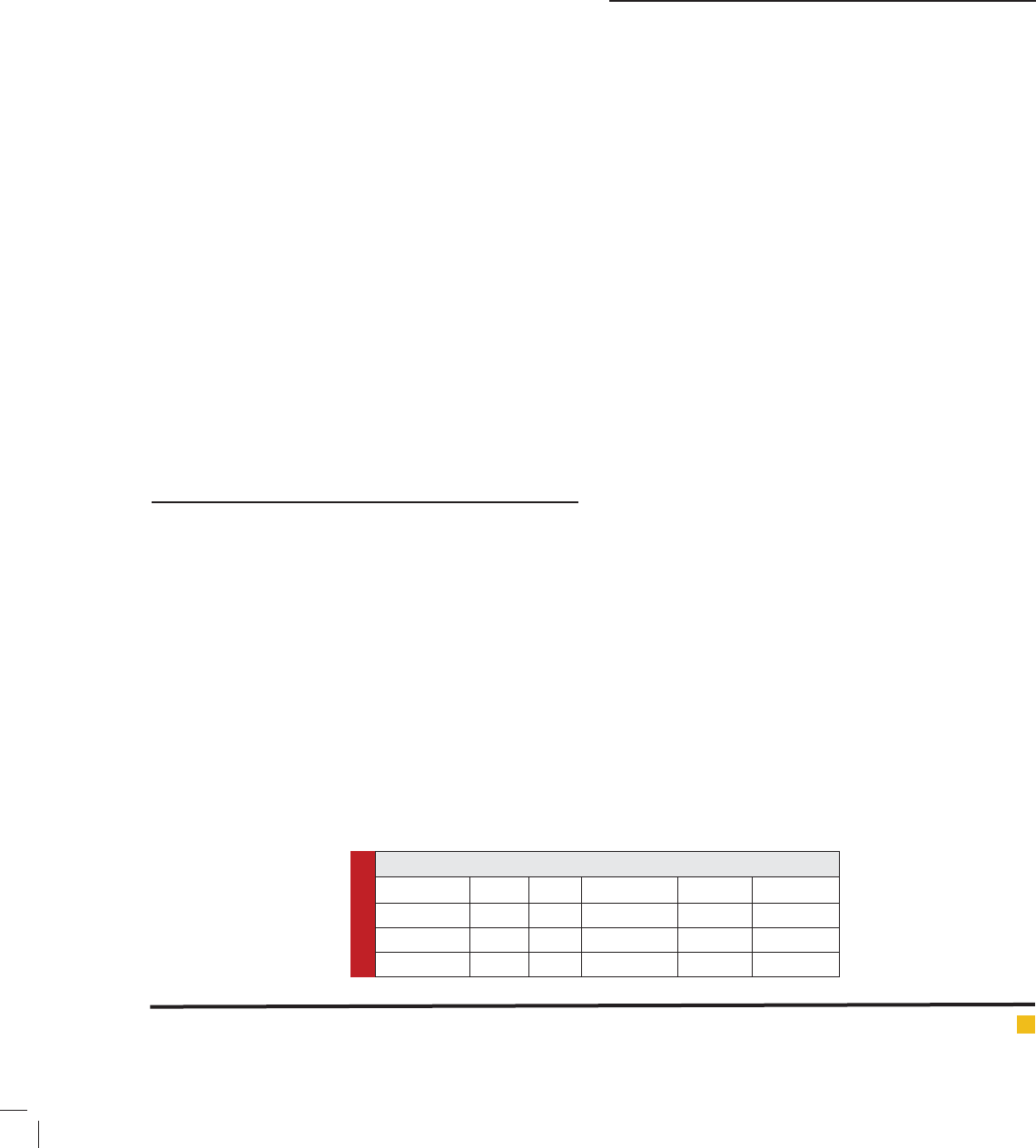
Table 1: Patient information
Sample ID AGE SEX Braak-NFT CERAD Infarction
496T 84 F 2.3 - +
691F 83 M 3.4 4 +
697P 87 M 4.4 6 +
endothelial cells and neurons through p-IRS-1, p-Tau
and p-ERK1/2-which was blocked following pre-incu-
bation with mCRP-antibody suggesting that the anti-
body could have therapeutic potential. mCRP increased
vascular monolayer permeability and gap junctions,
increased NCAM expression and produced haemorrhagic
angiogenesis in mouse matrigel implants and clearly has
abnormal effects on the vascular system.
Previously, Strang et al (2012) have demonstrated
that A plaques generated in vitro were able to dissoci-
ate pCRP to mCRP, probably produced de-novo within
the brain ECM, whilst in vivo, more mCRP was identi-
ed within frontal cortex regions in victims of AD than
normal control brains suggesting a possible pathological
or regulatory role in development of the disease. Cer-
ebrovascular disease, neurovascular dysfunction and
cerebral blood ow abnormalities are now recognised
as critical in uences in the pathophysiological devel-
opment of AD, damaged, blocked or in patent vessels
having a severe effect on the function of local neuro-
vascular units (with approximately 80% of AD brains at
post-mortem shown to have signi cant vascular abnor-
malities), in addition to Vascular dementia, and lowers
the threshold for development particularly in younger
patients, (Toledo, 2013 and Montagne 2016).
Here, in the present study, we have investigated the
possible link between mCRP deposition and localization
within the brain and indicators of previous stroke or
vascular disruption and dementia.
MATERIAL AND METHODS
Samples of brain tissue were obtained from the Bristol
Brain Bank, where from a cohort of 10 individuals, 3
were identi ed as having concomitant histological evi-
dence of AD and stroke (assessed independently and also
by our clinical neurologist; Table 1), and a clinical reg-
istered history of AD. The AD cases all had a history of
progressive dementia and were selected on the basis of a
diagnosis according to CERAD of ‘de nite AD’ (Hyman
2012). AD neuropathological change was considered a
suf cient explanation for the dementia in all cases.
Paraf n processed sections from frontal parietal and
temporal regions were examined for expression of mCRP
and in addition co-staining (double immunohistochemi-
cal labelling with VIP-vector kits) for key marker pro-
teins of neurodegeneration (p-Tau and -amyloid).
Particular attention was given to analysis of staining
patterns associated with areas of tissue showing evi-
dence of in ammation, vascular damage and regions
showing morphological appearance of micro-infarct or
other previous stroke.
RESULTS AND DISCUSSION
The staining pattern revealed that mCRP was almost
absent from normal looking regions of brain tissue with-
out signs of neurodegeneration or previous tissue insult.
Occasional blood vessels, neurons and glia of brain tis-
sue showed positive mCRP staining. However, mCRP
expression increased in the areas demonstrating typical
AD pathology (i.e. amyloid deposits and neuro billary
tangles). In these later areas, mCRP was mainly localized
to blood vessels and neurons with a smaller expression
within glia. Since these areas were not associated with
previous infarction, the expression of mCRP is likely to
be de novo synthesis similar to that seen by Strang et al
[Strang 2012], however, within blood vessel walls, mCRP
could in ltrate from the circulation through damaged
intimal linings.
mCRP expression was most abundantly present in
areas of microinfarction (and adjacent regions) in both
grey and white matter, whilst in relatively normal looking
areas, expression was weak or none-existent (Figure 1A).
mCRP expression was not seen in normal looking
regions and hence quanti cation of the extent of stain-
ing was not attempted. This is in line with our previ-
ously published observation and hypothesis of a direct
link between mCRP deposition and vascular damage
in the brain linking it to subsequently and chronically
hypo-perfused tissue regions [Slevin 2010].
B-amyloid staining and co-localization: Areas with
evidence of previous microinfarctions concomitantly
expressed more -amyloid. -amyloid deposition may
increase because of chronic in ammation after stroke
associated with chronic cerebrovascular dysfunction,
and this could be perpetuated at least in part by the
presence of excessive mCRP (Humpel 2011,Thiele, 2014
and McCaulley 2015).
Similarly, build-up of -amyloid is known to induce
neuro-in ammation directly, thus potentially perpetuat-
ing the neurodegenerative consequences (Hyman, 2012).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS C-REACTIVE PROTEIN AS EVIDENCE OF LOCALISED NEURODEGENERATIVE DISEASES 367
Hsinawi and Baradie
Hsinawi and Baradie
Some of the amyloid plaques were close to adjacent
blood vessels where mCRP expression was abundant
(Figure 1B). Since mCRP is known to stimulate aber-
rant angiogenesis (Selvin, 2014), this expression could
have a potential negative in uence on existing or neo-
microvessel function and patency contributing to pro-
duction of a local hypo-perfusive neurodegenerative-
friendly environment.
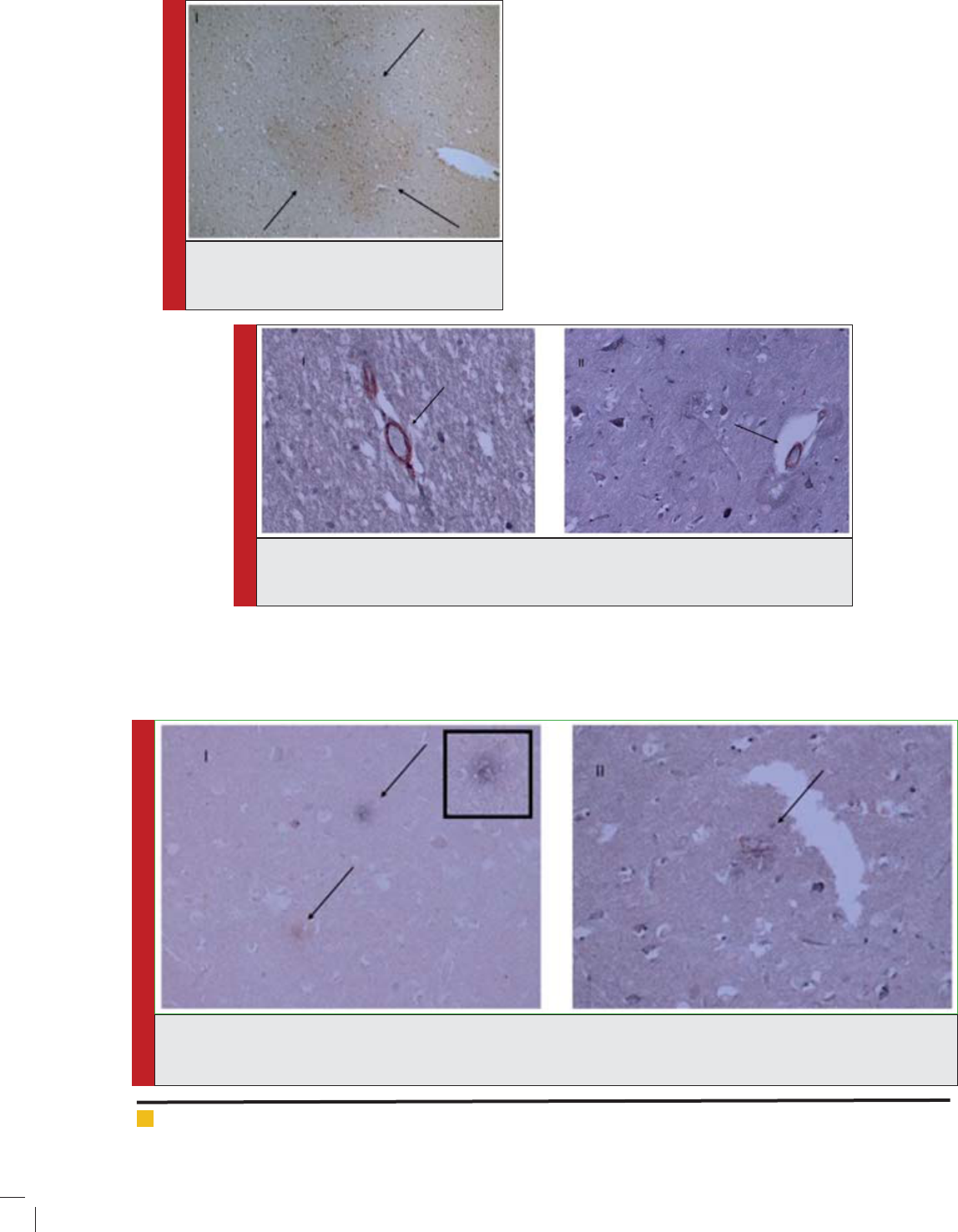
The co-localization between mCRP and -amyloid in
blood vessels was also mainly seen within areas or adja-
cent to small infarcts (Figure 1B); however, it was also
observed sporadically in other areas of pure tau pathol-
ogy without clear infarction in the area.
-amyloid pathology within existing plaques was
mainly separate, with mCRP-positive ‘plaque’-like mate-
FIGURE 1. Single staining for mCRP-showing
increased expression within a micro-infarcted
area (496T; arrows; x 100)
FIGURE 2. Double labelled sections from previously infarcted regions of white (i) and grey
(ii) matter showing co-localization of -amyloid (red) with mCRP (blue-black) (691F; x
200; arrows).
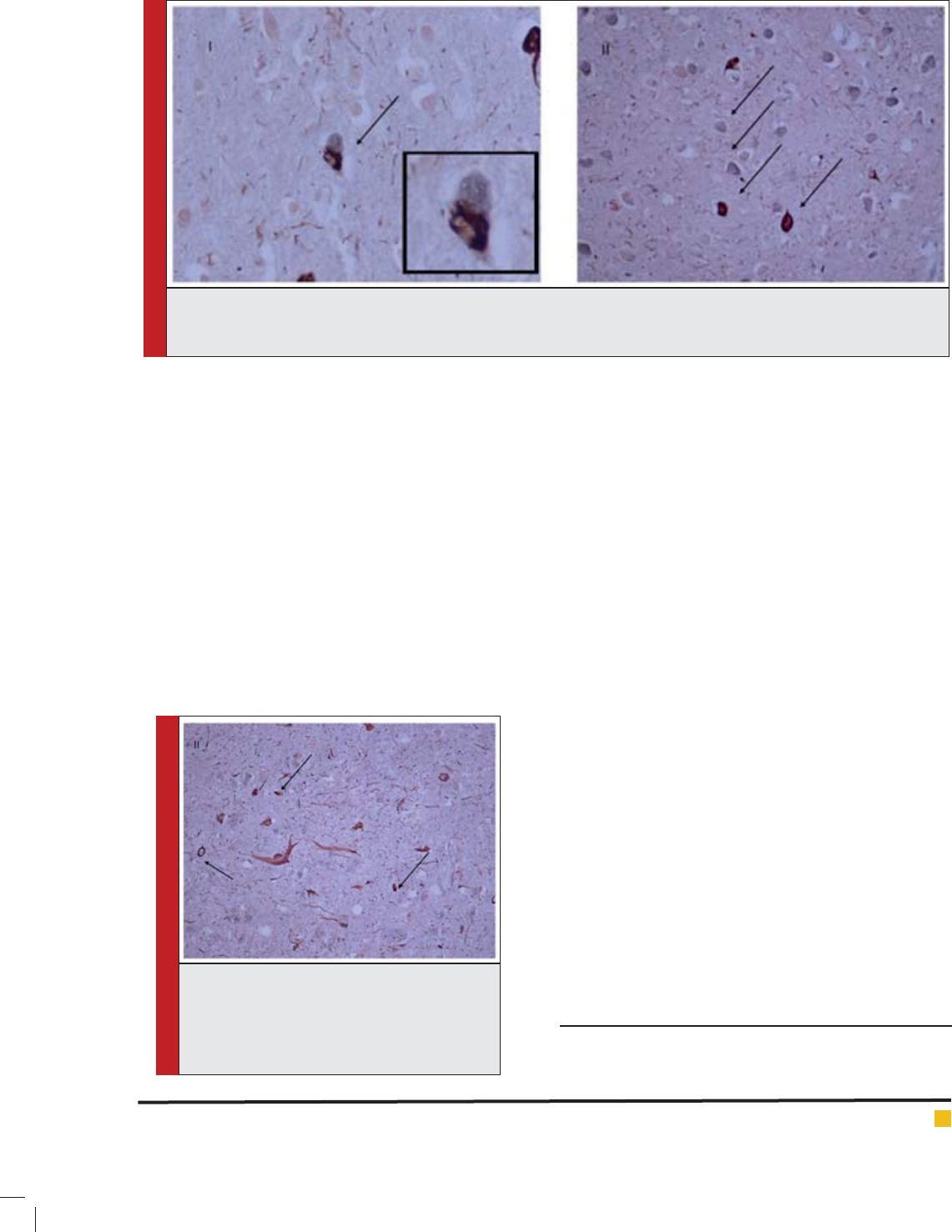
FIGURE 3. Double staining for -amyloid and mCRP showing (i) -amyloid-positive (red) and mCRP-positive (blue-black)
separate plaques in none-infarcted regions (ii) a plaque containing both proteins within a previously infarcted area (arrows).
(697P; x 100 (inset x 200) (i) and x 200 (ii)).
rial generally being distinct from regular AD plaques, in
relatively normal looking tissue regions. However, adja-
cent to previously infarcted regions some of the plaques
(approximately 10% based on counting of 10 x elds
of view at x 100 per section of 3 sections) contained a
combination of the two proteins (Figure 1C).
p-Tau staining and co-localization: The majority of
infarcted areas also exhibited other typical AD pathol-
368 C-REACTIVE PROTEIN AS EVIDENCE OF LOCALISED NEURODEGENERATIVE DISEASES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Hsinawi and Baradie
ogy like Tau deposits. Most of the mCRP co-localized pri-
marily with Tau within neurons in peri-nuclear regions
(Figure 1D), although, again, the majority of neurons
were either p-Tau or mCRP positive however the num-
ber of neurons co-localising with the two proteins was
approximately (15% based on counting of 10 x elds of
view at x 100 per section of 3 sections). Localization of
mCRP with phosphorylated tau in neurons could have
physiological signi cance.
Ourselves and others have demonstrated that mCRP
can phosphorylate tau (Ser 202,396) directly in vitro
(Selvin 2015; Guo 2015), possibly by a mechanism
involving GSK3. It is worthy of note that whilst co-
localising, the two proteins mCRP and p-Tau were pre-
sent generally at different positions within the neurons.
Toxic Tau brils (neuro brillary tangles) were present
in some of the most degenerated regions and there was
evidence of co-localization of p-Tau with mCRP here
also suggesting as our previous work showed that mCRP
could contribute or perpetuate to their development
(arrows showing dark grey staining) potentially impli-
cating mCRP in its development (Figure E).
Limitations of this ‘case study’ analysis are clearly
from the small numbers of sections and patients
reviewed. In addition, the relative timing of events in
these patients e.g. infarction versus AD symptoms is not
known and so the relative in uence of one process on
the other is subjective.
Given its strong aberrant biological properties associ-
ated with neurodegenerative signalling, vascular modu-
lation and angiogenesis, and its direct perpetuation of
in ammatory responses, a clear role for this protein in
promoting AD and VaD is proposed (Slevin, 2009). The
ndings shown here strengthen this hypothesis further
providing case studies of AD patients where vascular
insults probably linked to a local hypoxic environment
appear to be highlighted by a strong deposition of mCRP
and concomitant disproportionate evidence of localised
neurodegenerative disease. Since the majority of patients
who suffer serious stroke go on to develop cognitive
decline, lower executive function, and psychomotor pro-
cessing speed; and over 10% AD within 5 years (Desmond,
2002 and Mandzia, 2016), further research should study
potential mechanisms linking the two conditions with a
view to creating protective novel therapeutics.
CONCLUSION
mCRP is not found in normal-looking brain tissue of non
dementia patients, however it is produced and laid down
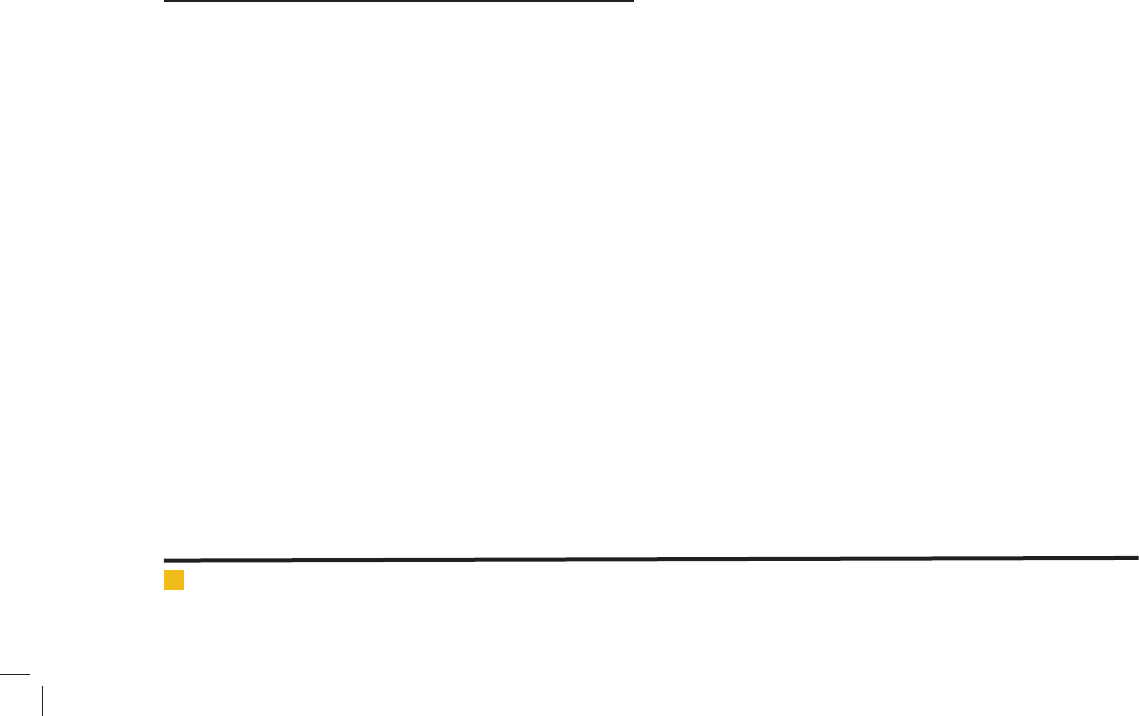
FIGURE 4. Double staining co-localization within micro-infarcted areas of p-tau (red) and mCRP (blue-black) (i) an iso-
lated double-labelled neuron (x 100; inset x 200) and (ii) neurodegenerative grey matter with separately stained neurons
for mCRP and p-Tau (arrows).
FIGURE 3. Double staining showing co-local-
ization of amyloid and mCRP (blue-black)-
NFTs-p-Tau (red) in an infarcted grey matter
brain region. (i) areas of co-localization are
shown by arrows (691T; x 200).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS C-REACTIVE PROTEIN AS EVIDENCE OF LOCALISED NEURODEGENERATIVE DISEASES 369
370 C-REACTIVE PROTEIN AS EVIDENCE OF LOCALISED NEURODEGENERATIVE DISEASES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Hsinawi and Baradie
in large quantities within the brain following stroke, other
brain injury or conditions linked with neuro-in amma-
tion. We hypothesise that vascular disruption and con-
comitant release of mCRP within the brain tissue could
exacerbate ongoing neurological damage via stimulation
of neuro-in ammation and from direct consequences of
its action on both neuronal and vascular health.
DECLARATIONS-NONE
Abbreviations used: mCRP-Monomeric C-reactive
protein; VaD-Vascular dementia; AD-Alzheimer’s dis-
ease; ECM-Extra cellular matrix; CERAD-Consortium to
establish a registry for Alzheimer’s disease.
Ethics approval and consent to participate: Full ethi-
cal approval was obtained for the use of tissue sam-
ples as detailed by the South West Dementia Brain Bank
(SWDBB) and obtained from them.
Consent for publication: Has been obtained by all
authors
Availability of data and materials: N/A
Competing interests: The authors declare they have no
competing interests
Funding: This work was supported by the Research Cen-
tre of Healthcare Science at Manchester Metropolitan
University, and by Sheikh Abdullah bin Abdul Mohsen
Al-Tuwaijri project grants within, Majmaah University,
Saudi Arabia
ACKNOWLEDGEMENTS
We would like to thank the South West Dementia Brain
Bank (SWDBB) for providing brain tissue for this study.
The SWDBB is part of the Brains for Dementia Research
programme, jointly funded by Alzheimer’s Research UK
and Alzheimer’s Society and is supported by BRACE
(Bristol Research into Alzheimer’s and Care of the
Elderly) and the Medical Research Council.
This research was supported by Sheikh Abdullah
bin Abdul Mohsen Al-Tuwaijri project grants within,
Majmaah University, Saudi Arabia. The authors would
like to express their gratitude towards Sheikh Abdullah
Abdul Mohsen Al-Tuwaijri, Rector Dr. Khalid Saad Al
Muqrin for providing the necessary support and assis-
tance in completing this piece of work.
REFERENCES
Desmond DW, Moroney JT,Sano M, Stern Y (2002), Incidence
of Dementia After Ischemic Stroke: Results of a Longitudinal
Study. Stroke. (33):2254-2262.
Hyman BT, Phelps CH, Beach TG, Bigo EH, Cairns NJ, Carrillo
MC, Dickson DW, Duyckaerts C, Frosch MP, Masliah E, Mirra
SS< Nelson PT, Scneider JA, Thal DR, Thies B, Trojanowski JQ,
Vinters HV, Montine TJ (2012) National Institute on Aging–
Alzheimer’s Association guidelines for the neuropathologic
assessment of Alzheimer’s disease. Alzheimer’s Dementia. 8(1):
1-13.
Guo H, Wang H, Wang C, Cheng Y, Zou Z, Li Y, Wu J, Xu J
(2015). C-Reactive Protein Induces Tau Hyperphosphorylation
via GSK3 Signaling Pathway in SH-SY5Y Cells. J Mol Neu-
rosci. 56(2):519-27.
Humpel C (2011) Chronic mild cerebrovascular dysfunction for
Alzheimer’s disease? Exp. Gerentol. 46(4): 225-232.
Mandzia JL, Smith EE, Horton M, Hanly P, Barber PA, God-
zwon C, Donaldson E, Asdaghi N, Patel S, Coutts SB (2016).
Imaging and Baseline Predictors of Cognitive Performance in
Minor Ischemic Stroke and Patients With Transient Ischemic
Attack at 90 Days. Stroke. 47(3):726-31.
McCaulley ME, Grush KA (2015) Alzheimer’s Disease: Explor-
ing the Role of In ammation and Implications for Treatment.
Int J Alzheimers Dis. Epub 2015 Nov 17.
Montagne A, Nation DA, Pa J, Sweeney MD, Toga AW, Zloko-
vic BV (2016) Brain imaging of neurovascular dysfunction in
Alzheimer’s disease. Acta Neuropathol. In press.
Slevin M, and Krupinski J (2009) A role for monomeric
C-reactive protein in regulation of angiogenesis, endothelial
cell in ammation and thrombus formation in cardiovascular
disease? Histol. Histopathol. (2009) (24)11: 1473-1478.
Slevin M, Matou-Nasri S, Turu M, Luque A, Rovira N, Badi-
mon L, Boluda S, Potempa L, Sanfeliu C, de Vera N, Krupinski
J (2010). Modi ed C-reactive protein is expressed by stroke
neovessels and is a potent activator of angiogenesis in vitro.
Brain Pathol. 20(1):151-65.
Slevin M, Matou S, Zeinolabediny Y Corpas R,Weston R,Liu
D,Boras E,Di Napoli M,Petcu E, Sarroca S Popa-Wagner A, Love,
S, Font MA, Potempa LA, Al-baradie R, Sanfeliu C, Revilla
S, Badimon L, and Krupinski J (2015). Monomeric C-reactive
protein-a key molecule driving development of Alzheimer’s
disease associated with brain ischaemia? Sci. Rep. 2015:
13281.
Strang F, Scheichl A, Chen YC, Wang X, Htun NM, Bassler
N, Eisenhardt SU, Habersberger J, Peter K (2012). Amyloid
plaques dissociate pentameric to monomeric C-reactive pro-
tein: a novel pathomechanism driving cortical in ammation in
Alzheimer’s disease? Brain Pathol. 22(3):337-46.
Thiele JR, Habersberger J, Braig D, Schmidt Y, Goerendt K,
Maurer V, Bannasch H, Scheichl A, Woollard KJ, von Dob-
schütz E, Kolodgie F, Virmani R, Stark GB, Peter K, Eisenhardt
SU (2014). Dissociation of pentameric to monomeric C-reactive
protein localizes and aggravates in ammation: In vivo proof
of a powerful proin ammatory mechanism and a new anti-
in ammatory strategy. Circulation. (1):35-50.
Toledo JB, Arnold SE, Raible K, Brettschneider J, Xie SX,
Grossman M, Kukull WA, Trojanowski JQ (2013) Contribution
of cerebrovascular disease in autopsy con rmed neurodegen-
erative disease cases in the National Alzheimer’s coordinating
centre. Brain. (136):2697-2706.